INTRODUCTION
Maternal undernutrition is a significant concern in developing countries, especially of the South Asian region1. More than half of all women of reproductive age weigh less than 45 kg in this region2. Every year, more than 3.5 million women in developing countries die as a result of undernutrition3. Moreover, half of the world’s undernourished women are found in three developing countries including Bangladesh, India and Pakistan1. Maternal undernutrition has been identified as a serious issue in Pakistan. According to the National Nutritional Survey of Pakistan 2011, 50% of pregnant women in the country are anemic, 46% had vitamin A deficiency, while 47% and 68% were zinc and vitamin D deficient, respectively4.
Hence, undernutrition is a substantial underlying factor contributing to high maternal and childhood mortality in Pakistan and places an additional burden on the already limited resources of the country3. Since undernourished mothers are at higher risk of giving birth to underweight children, undernutrition can have a vicious, multigenerational impact5.
Studies have also demonstrated a close association between the mother’s nutritional status and various pregnancy outcomes such as low birthweight, susceptibility to infections, and growth-challenged and developmentally delayed children6,7. Numerous factors can predict the nutritional status of a woman such as conditional influences, food production, cultural factors, socioeconomic and fertility-related factors8. For example, the fertility rate in Pakistan is very high and, on average, one Pakistani woman gives birth to 3.8 babies. Out of all women belonging to the reproductive age group in the country, only 35% have been documented to use contraception9. A high fertility rate and lack of birth spacing result in a continuous cycle of pregnancy and lactation, which can deplete the nutritional reserves of an already undernourished mother. Hence, the parity of a woman and birth spacing have a significant impact on the child’s chances of survival3. A short inter-pregnancy interval does not give the mother sufficient time to recover from the birth process and replenish her stores of nutrients consumed during pregnancy, especially in the background of undernutrition10. Thus, too many (high parity) and too frequent pregnancies (shorter birth intervals) result in maternal undernutrition, which not only has an adverse effect on maternal health but also affects neonatal and infant health9. There is a dearth of research assessing the predictors of undernutrition status among women in Pakistan. The objective of this study was to assess the determinants of undernutrition among women of reproductive age in Sindh, Pakistan, using the national demographic health survey.
METHODS
The data of 4050 ever married women of reproductive age were extracted from a nationally representative sample, the Pakistan Demographic and Health Survey 2012–2013 completed by The National Institute of Population Studies (NIPS). The primary outcome variable was the nutritional status of the woman, which was dichotomized into a binary variable (undernourished and well nourished). The nutritional status of the women of reproductive age was determined using data on body mass index or BMI (kg/m2), which was categorized as <18.5 being ‘undernourished’ and ≥18.5 ‘adequately nourished.’ In addition, sociodemographic and fertility-related variables such as age, place of residence, educational status, working status, wealth index, contraceptive usage, intention of pregnancy, parity, birth order, breastfeeding, smoking status, and other relevant variables were identified as independent variables from the PDHS data for further analysis. Hence, these data were part of PDHS during which literate data collectors were hired who translated and administered the questionnaires to the participants. These data collectors asked all questions in the local language of the participants. Data from the PDHS were publicly available data on a national level, so there was no need of IRB approval for analysis of the objective assessed in the study. In addition, they were secondary data, largely available for the public to analyze and answer specific research questions, without a need of IRB approval. We did not select the subjects ourselves rather these were selected by following multistage cluster sampling across the country.
Statistical analysis
Data analysis was carried out using STATA version 12. Weighted analysis was done to obtain a representative sample in order to avoid over- or under-estimation by considering clusters, strata and sampling weights into the analysis for complex survey design. The normality of continuous data was assessed using histograms, p-p plots and by applying the Kolmogorov test. This was followed by computation of descriptive statistics for both continuous and categorical variables. Frequencies with percentages were calculated for the categorical variables including place of residence, women’s level of education, working status of the women, and use of contraceptive methods.
To identify the factors associated with undernutrition, univariable analysis followed by multiple logistic regression was carried out. For each independent variable, crude odds ratios and adjusted odds ratios with their 95% confidence intervals and p-values were calculated.
Analysis was done by a purposeful selection method and all the variables that were selected in the univariable analysis were entered in the model. The significance of each independent variable in the multivariable analysis was assessed by p<0.05.
RESULTS
Sociodemographic characteristics of women by nutritional status
Those aged 15–24 years comprised 8.6% undernourished women and 6% adequately nourished women. Similarly, there were 47.4% undernourished women aged 25–34 years compared with 30.3% adequately nourished, belonging to the same group (Table 1).
Table 1
Sociodemographic and fertility-related factors by nutritional status of women of reproductive age (N=4054)
With respect to the ethnicity of the women, 45.9% of the undernourished women were found to be Sindhi speaking, 8% were Urdu speaking, 0.6% spoke Punjabi, and 45.6% spoke other regional languages. With regard to place of residence, 80.5% of the undernourished women were from rural areas. With respect to education, 79.7% of the undernourished women were not educated and 2.1% had received education for ≥12 years (Table 1).
Amongst the undernourished group, 45.1% women were working while 72.6% lived below the poverty line. Regarding the type of fuel used by the women, 19.3% of the undernourished women reported that they used gas for cooking as the primary type of fuel while 55.1% reported using either charcoal or wood. As for smoking, 4.8% of the undernourished women were found to be cigarette smokers, of these, 7.2% also reported tobacco chewing. With regard to knowledge about tuberculosis, 97% of the undernourished women had heard of the disease. Additionally, 39.4% of the undernourished women reported using a mosquito bed net for sleeping (Table 1).
Fertility-related factors of participants by nutritional status of the woman
With respect to parity, 44% of the undernourished women had ≤4 children while 56% had ≥5 children. Of the undernourished women, 38% reported using contraceptives while 97.1% reported at least one unwanted pregnancy. As for breastfeeding, 40.5% of the undernourished women reported that they breastfeed their child (Table 1).
Determinants of undernutrition: Findings of univariable analysis
Sociodemographic factors
We found that younger women were 2.41 times more likely to be undernourished compared to older women (OR=2.41; 95% CI: 1.68–3.45). Women with no formal education were 5.25 times more likely to be undernourished compared to women who had received formal education (OR=5.25; 95% CI: 3.04–9.07). Similarly, working women were 1.73 times more likely to be undernourished compared to non-working women (OR=1.73; 95% CI: 1.47–2.05). Those residing in rural areas had 4.01 times greater odds of being undernourished compared to women from urban areas (OR=4.01; 95% CI: 3.27–4.92). Women living below the poverty line were 4.56 times more likely to be undernourished compared with those who were financially well to do (OR=4.56; 95% CI: 3.68–5.72). Those who smoked had a 4.90 times greater likelihood of being undernourished compared to non-smokers (OR=4.90; 95% CI: 3.01–7.97) (Table 2).
Table 2
Association between sociodemographic characteristics with undernutrition among married women of reproductive age (N=4054)
| Characteristics | OR | 95% CI | p* |
|---|---|---|---|
| Age (years) | <0.001 | ||
| 15–24 | 2.41 | 1.68–3.45 | |
| 25–34 | 2.62 | 2.06–3.34 | |
| 35–44 | 1.27 | 0.98–1.64 | |
| ≥45 | 1 | ||
| Education level | <0.001 | ||
| Intermediate and above | 1 | ||
| Middle to secondary | 1.59 | 0.82–3.05 | |
| Primary education | 4.83 | 2.69–8.67 | |
| No education | 5.25 | 3.04–9.07 | |
| Literacy | <0.001 | ||
| Literate | 1 | ||
| Illiterate | 2.04 | 1.63–2.46 | |
| Working status | <0.001 | ||
| No | 1 | ||
| Yes | 1.73 | 1.47–2.05 | |
| Place of residence | <0.001 | ||
| Urban | 1 | ||
| Rural | 4.01 | 3.27–4.92 | |
| Ethnicity | <0.001 | ||
| Urdu | 1 | ||
| Punjabi | 0.38 | 0.14–1.07 | |
| Sindhi | 3.42 | 2.52–4.65 | |
| Other | 3.11 | 2.29–4.23 | |
| Wealth index | <0.001 | ||
| Rich | 1 | ||
| Middle | 3.17 | 2.32–4.34 | |
| Poor | 4.56 | 3.68–5.72 | |
| Type of cooking fuel | <0.001 | ||
| Gas | 1 | ||
| Charcoal/wood | 3.97 | 3.20–4.91 | |
| Straw/animal dung | 4.93 | 3.82–6.36 | |
| Other | 5.02 | 2.46–10.24 | |
| Smoking cigarettes | <0.001 | ||
| No | 1 | ||
| Yes | 4.9 | 3.01–7.97 | |
| Chew tobacco | >0.05 | ||
| No | 1 | ||
| Yes | 0.95 | 0.69–1.30 | |
| Heard of tuberculosis | <0.001 | ||
| No | 1 | ||
| Yes | 0.39 | 0.23–0.68 | |
| Mosquito bed net for sleeping | <0.001 | ||
| Yes | 1 | ||
| No | 0.45 | 0.38–0.53 |
Fertility-related factors
Women with ≥5 children were 33% less likely to be undernourished compared to women having <5 children (OR=0.67; 95% CI: 0.56–0.78). Those with intended pregnancies were 2.58 times more likely to be undernourished compared with those with an unintended pregnancy. Women breastfeeding their children were 1.87 times more likely to be undernourished compared to women who did not breastfeed (OR=1.87; 95% CI: 1.57–2.22) (Table 3).
Table 3
Association of fertility-related factors with undernutrition among married women of reproductive age (N=4054)
| Characteristics | OR | 95% CI | p* |
|---|---|---|---|
| Currently pregnant | <0.001 | ||
| Yes | 1 | ||
| No | 1.8 | 1.22–2.67 | |
| Parity | <0.001 | ||
| 0–4 | 1 | ||
| ≥5 | 0.67 | 0.56–0.78 | |
| Contraceptive use | <0.001 | ||
| Yes | 1 | ||
| No | 0.90 | 0.76–1.07 | |
| Pregnancy intention | <0.001 | ||
| No | 1 | ||
| Yes | 2.58 | 1.61–4.13 | |
| Fertility preference | <0.001 | ||
| Wants another child | 1 | ||
| Does not want another child | 0.66 | 0.55–0.79 | |
| Breastfeeding | <0.001 | ||
| Yes | 1 | ||
| No | 1.87 | 1.57–2.22 |
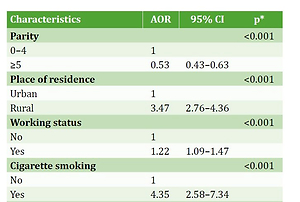
Determinants of undernutrition: Findings of multivariable analysis
The multivariable analysis found that women having ≥5 children were 47% less likely to be undernourished compared to women having <5 children (AOR=0.53; 95% CI: 0.43–0.63). Those from rural areas were 3.47 times likely to be undernourished compared to women from urban areas (AOR=3.47; 95% CI: 2.76–4.36). Similarly, working status increased the likelihood of undernutrition by 1.22 times (AOR=1.22; 95% CI: 1.09–1.47). Women who smoked cigarettes were 4.35 times likely to be undernourished compared to those who did not smoke (AOR=4.35; 95% CI: 2.58–7.34). Non-pregnant women were 2.22 times more likely to be undernourished compared to pregnant women (AOR=2.22; 95% CI: 1.46–3.30). Women who breastfed were 1.40 times more likely to be undernourished compared to women not breastfeeding their children (AOR=1.40; 95% CI: 1.16–1.68) (Table 4).
Table 4
Determinants of undernutrition among women of reproductive age (N=4054)
| Characteristics | AOR | 95% CI | p* |
|---|---|---|---|
| Parity | <0.001 | ||
| 0–4 | 1 | ||
| ≥5 | 0.53 | 0.43–0.63 | |
| Place of residence | <0.001 | ||
| Urban | 1 | ||
| Rural | 3.47 | 2.76–4.36 | |
| Working status | <0.001 | ||
| No | 1 | ||
| Yes | 1.22 | 1.09–1.47 | |
| Cigarette smoking | <0.001 | ||
| No | 1 | ||
| Yes | 4.35 | 2.58–7.34 | |
| Heard of tuberculosis | <0.001 | ||
| Yes | 1 | ||
| No | 2.14 | 1.18–3.90 | |
| Mosquito bed net for sleeping | <0.001 | ||
| Yes | 1 | ||
| No | 0.638 | 0.52–0.77 | |
| Pregnant | |||
| Yes | 1 | ||
| No | 2.22 | 1.46–3.30 | |
| Breastfeeding | |||
| No | 1 | ||
| Yes | 1.4 | 1.16–1.68 |
DISCUSSION
This data analysis from cross-sectional, nationally representative surveys conducted throughout the province of Sindh, Pakistan, provides evidence for relationships between parity and other socioeconomic and fertility-related factors with the nutritional status of women.
It demonstrates that parity is protective against undernutrition, as women with ≥5 children were less likely to be undernourished compared with women with <5 children. Our findings are consistent with studies conducted in Mexico, North Africa/West Asia and China, where a weak to moderate positive association was found between parity and increased BMI11,12. These findings can be explained by the fact that cumulative cycles of post-partum weight retention are the primary mechanism by which parity leads to increased BMI13,14. Literature shows that the excess gestational weight gain can lead to post-partum weight retention and has been associated with increased weight gain in the long-term15,16. Lifestyle factors, including physical activity and dietary intake in the post-partum period can also be associated with post-partum weight retention, which in turn, determines the nutritional status of the mother. In addition to this, women with low parity might also be younger compared to those with high parity, which is consistent with our finding of younger women being more undernourished compared with older women.
These findings of a relationship between parity-related weight and nutritional status suggest a need for the development and implementation of programs to prevent and treat parity-related obesity in developing countries. Such programs could include efforts to prevent post-partum weight retention by promoting exclusive breastfeeding concomitant with moderate levels of physical activity. Moreover, younger women with low parity should be targeted for counseling regarding balanced and adequate diet to improve their nutritional status.
With respect to the place of residence, it was found that women living in rural areas were more likely to be undernourished compared to women belonging to urban areas. This finding is consistent with other studies conducted across the world17-19. Widespread poverty and lower socioeconomic conditions in rural areas might be possible factors that explain the high prevalence of undernutrition among women of reproductive age. For instance, undernutrition has been significantly associated with various factors like unskilled labor, financial constraints, overcrowding, households without electricity and tap water. These are also some of the major problems faced by women residing in rural areas19.
It is recommended that programs be designed to improve the nutritional status of women living in remote areas of Pakistan. During the past few years, many nutritional programs have been initiated by governmental and nongovernmental organizations20. Some of these programs focus on raising awareness among the population, while others focus on either directly supplying nutrients or fortification of dietary components. However, the root causes of the problem like illiteracy, poverty, and socioeconomic deprivations, are still being neglected21.
With regard to occupation, working women were more likely to be undernourished compared to non-working women of reproductive age. These findings might be due to the fact that working mothers have a greater energy expenditure that contributes to a lower bodyweight and BMI. However, literature supporting this evidence is very scarce, but these findings are consistent with the study conducted in Bangladesh, where females who worked 15–23 days per month had significantly better BMIs than those who worked >23 days per month19. These findings were inconsistent with the study conducted in Marzi Pura Faisalabad, Pakistan, where it was found that working status had a positive association with adequate nutrition and BMI22. These differences in findings may be because of the differences in study setting, sample size, and study population.
With respect to smoking status, women who smoked were more likely to be undernourished compared to nonsmokers. This finding can be explained by the biological fact that smoking reduces appetite and provides satiety. These findings are consistent with a study conducted in Styria, in southeast Austria23. Thus, one might expect that women who smoke would be more undernourished because of their poor appetite and diet. Moreover, smokers are more likely to indulge in other activities like tobacco chewing, bidi or huka use, which in turn deteriorate their nutritional status compared to their non-smoking counterparts. These women should be targeted for continuous counseling, and strategies need to be designed to alter the behavior of these women, not only to improve their nutritional status but also the nutritional status of their children.
With respect to breastfeeding, it was found that women who were breastfeeding their children were also more likely to be undernourished compared to the women not breastfeeding their children. These findings are in line with studies across the world that have found that breastfeeding contributes to maternal undernourishment24. This is a significant finding for women belonging to rural areas that do not have access to a balanced diet and have high fertility rates. Therefore, their body reserves are not adequately replenished, which creates a vicious circle of undernutrition8.
The public health implications of these findings depend on the context; greater maternal weight losses may be beneficial in healthy populations where women are already sufficiently nourished and they have access to a balanced diet, but detrimental in undernourished populations where women are mostly undernourished due to multiple causes like illiteracy, poverty, and lack of access to a nutritious diet. It is recommended that women who breastfeed their children take in extra calories to replenish their body reserves to prevent undernutrition8. Hence, these mothers should be adequately counseled about the intake of a balanced diet while breastfeeding their children.
It was also found that non-pregnant mothers were more likely to be undernourished compared to the pregnant mothers. These findings might be because of the physiological weight gain during pregnancy. Moreover, traditionally, Pakistani women who are pregnant are culturally encouraged to consume more calories compared to those who are non-pregnant. This may also explain the above finding of a good nutritional status during pregnancy. Although pregnancy increases the weight of the mother and pregnant women also tend to consume more calories during pregnancy, a balanced diet is also equally important for women who are married but not pregnant. Married and nonpregnant women are in their preconception phase, which is considered the right time to start adequate nutrition25,26. Studies have also found that maternal undernutrition during the first trimester of pregnancy carries the greatest risk for fetal development and so correcting nutritional status in early pregnancy is likely to yield the greatest benefits for both the mother and the offspring25,26. Thus, adequate nutrition should be provided to women during the preconception period to avoid short-term and long-term adverse maternal and neonatal outcomes.
Strengths and limitations
This data analysis was conducted on a large and nationally representative sample of women in Pakistan using the PDHS 2012–2013. Hence, the findings can be generalized to the Pakistani population as well as to other regional countries that share similar sociodemographic characteristics.
Moreover, the survey covered various sociodemographic and health-related variables, which were analyzed to measure the association between parity and women’s nutritional status while adjusting for confounders. Additionally, weighted analysis was done to obtain representative estimates and to avoid under- or overestimation while analyzing the data.
One limitation of the study is its cross-sectional nature. Therefore, any association between the various predictors, especially parity and nutritional status, needs to be interpreted cautiously. Secondly, a key limitation of our study was the use of BMI as the only measure of nutritional status, which might not predict the true nutritional status of the women. Thus, stronger observational and analytical studies need to be carried out in the future to assess the association between parity and other predictors of nutritional status in women.
CONCLUSIONS
Women who breastfed, worked, smoked, or belonged to rural areas were found to be the most undernourished. Our analysis suggests that undernutrition is likely to occur when women do not have access to a balanced diet and this can be determined from their place of residence, breastfeeding and pregnancy status, as well as whether or not they work. We recommend that rural women who breastfeed their children, as well as work, be targeted for awareness on balanced nutrition. The proximal as well as distal or root causes of undernutrition need to be explored and addressed in the future to improve the nutrition of women of reproductive age.