INTRODUCTION
Tobacco use is initiated and established mostly during adolescence1. Adolescence is a developmental period that is characterized by risk-taking and impulsive behavior. Peer influence is a dominant psychosocial issue, and the desire to conform increases adolescents’ vulnerability to elevated risk of health-compromising behaviors2. Adolescents’ tobacco use has immediate adverse health effects, including addiction, and increases the risk of developing major chronic diseases throughout the lifespan1.
Data from the 2012 to 2015 Global Youth Tobacco Survey (GYTS) for students aged 13–15 years show that the median current tobacco smoking prevalence was 10.7%; 14.6% among males and 7.5% among females3. The 2010 GYTS data for Saudi Arabia suggest a higher prevalence of youth tobacco use than the global prevalence, where 14.9% were current tobacco smokers; 21.2% males and 9.1% females4. Α few local studies in Saudi Arabia surveyed tobacco use among female adolescents and reported similar findings. The prevalence of tobacco use was reported to be 7% in middle school (13–15 years) female students in Jeddah5, 9% in high school (16–18 years) female students in Riyadh6, and 11% and 5% in both middle and high school female students from Tabuk and Taif, respectively7,8.
Although the reported tobacco use is significantly higher among males compared to females in Saudi Arabia, there are reasons for concern that tobacco use among females may be on the rise. Social norms in the Middle East and North Africa (MENA) region have historically stigmatized tobacco use among women and perceived it to be shameful. However, these norms have changed in the past decade with urbanization and the increasing numbers of cafés and restaurants that serve waterpipe tobacco9. Studies that examined gender differences in tobacco use among adolescents in Saudi Arabia found that female adolescents generally have less knowledge about the adverse health effects of tobacco use and hold significantly more positive attitudes towards tobacco use, compared to males. They also reported less tobacco education in female schools and lack of parental guidance in regard to smoking, which can be attributed to the misleading cultural perception that female adolescents are less likely to smoke than their male counterparts7,10. Additionally, tobacco prevention programs administered by the Department of Education in Saudi Arabia are exclusively offered to male schools, leaving female students at a disadvantage regarding the essential knowledge and skills needed to abstain from or quit tobacco use.
Schools provide an ideal setting for adolescent health promotion programs11. Programs to prevent tobacco use among youth apply a variety of models including informational intervention, social competence, social influence, and multimodal programs11. Informational intervention stresses the harmful physical and social consequences of tobacco use. The social competence model emphasizes effective education by teaching generic self-management and social skills such as goal-setting, problem-solving, and decision-making. The social influence model addresses normative beliefs, raises awareness about peer, family, and media influences, and teaches skills to confidently refuse such influences. Thomas and Perera12, in their systematic review of school-based smoking prevention studies, reported that information-only interventions did not produce the intended effect, whereas interventions that use social competence and influence models found significant positive results. However, evidence of a long-term impact on smoking prevalence was unclear12.
The Theory of Planned Behavior (TPB), proposed by Ajzen13, is an extension of the Theory of Reasoned Action that links the beliefs of individuals with their behavior. The theory states that behavioral, normative, and control beliefs collectively shape an individual’s behavioral intentions and behaviors. In this study, we developed and evaluated a comprehensive tobacco prevention program using the TPB to prevent tobacco use among seventh grade female students in Jeddah, Saudi Arabia. The findings of this study may validate or suggest policies and health promotion programs for tobacco prevention among Saudi female adolescents.
METHODS
Study sample
A quasi-experimental controlled design was utilized to test the feasibility of a school-based tobacco program, Dentist Fighting Nicotine Dependence (DFND), in preventing the initiation of tobacco use among female middle school students in Jeddah, Saudi Arabia. Middle school in Saudi Arabia starts in grade 7 and ends in grade 9. The students in grade 7 are typically 12–13 years old. This age represents a heightened vulnerability to tobacco use; more than a third of adults who have ever smoked tried their first cigarette at the age of 1414. The program targeted 7th grade students to facilitate the study of the same cohort for two consecutive years.
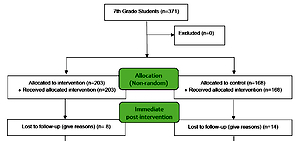
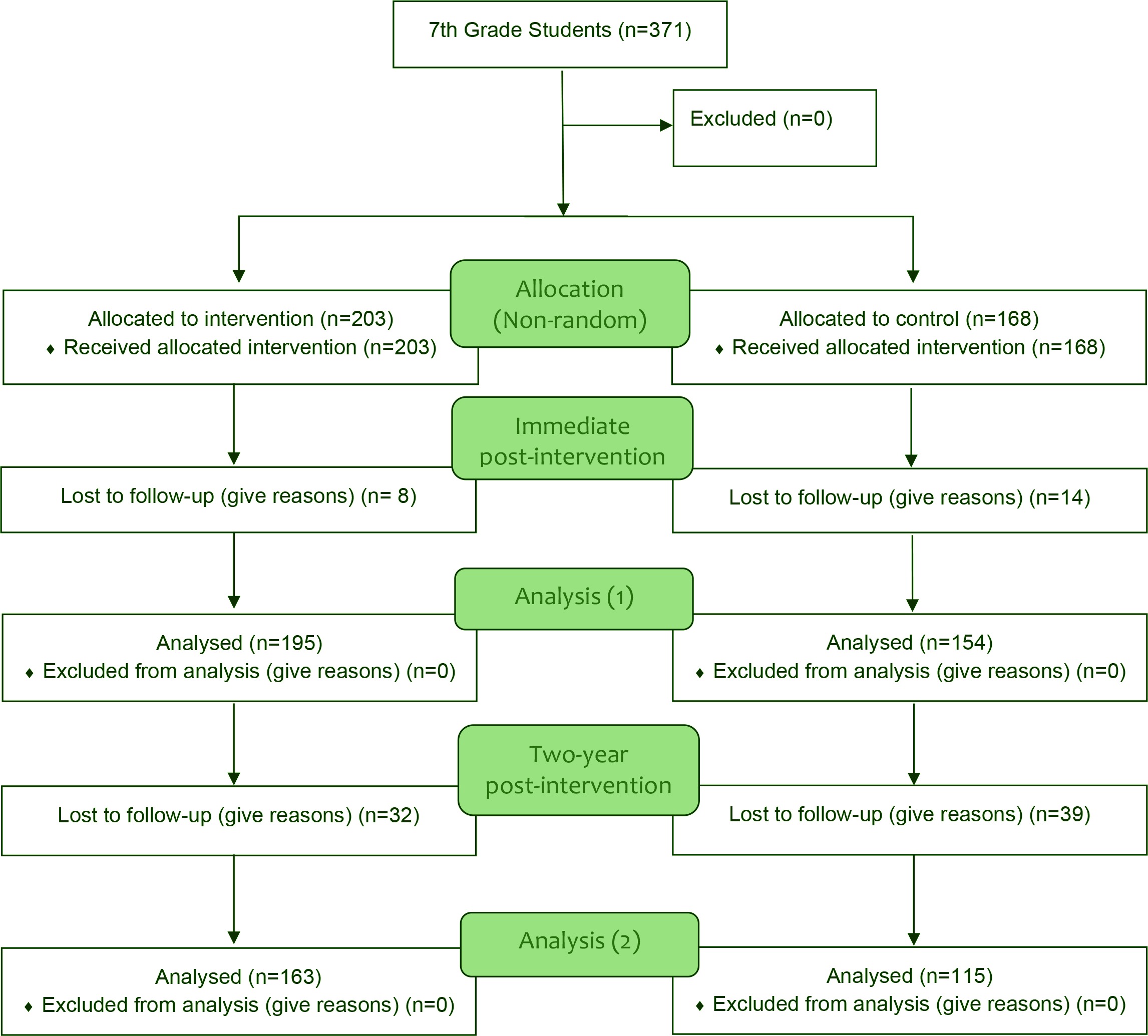
Four schools with similar sociodemographic characteristics, two intervention and two control were selected by the regional directors of education from the school registry in Jeddah. The intervention schools received the new tobacco prevention program, the DFND program, while the control schools only received an informational booklet about smoking and its adverse social and health effects and an anti-smoking poster for the school. Four 7th grade classes from each school were selected, enrolling a total of 16 classes in the study. Figure 1 illustrates the enrollment of study participants into intervention and control groups. The study commenced in February 2012 and was completed in April 2014.
School-based tobacco prevention program (DFND)
The DFND program is composed mainly of a series of tobacco educational modules and additional supportive components. The modules were taught in 10 interactive sessions that utilized lectures, videos, small group discussions, role play, and class assignments. The basic content of the program was adopted from a variety of American school-based tobacco prevention programs, which were modified to include tailored educational materials and tools to make it better suited for adolescents in Saudi Arabia15. The original DFND protocol also included two additional tobacco prevention sessions to be administered when the students were promoted to the 8th grade. However, we were unable to conduct them as planned.
The comprehensive curriculum integrated information about tobacco and its negative health effects, social influences, and social competence skills. The first session was informational and presented the different types and contents of tobacco products, prevalence of use, and the physical, social, and economic consequences of tobacco use. The second session addressed why adolescents use tobacco and highlighted personal, social, environmental, and cultural factors that encourage initiation of tobacco use. The third session uncovered common strategies and channels employed by the tobacco industry to market tobacco to youth. The fourth session explored factors that discourage quitting tobacco and discussed misconceptions about tobacco use. The fifth session discussed the biological, psychological, and social types of tobacco dependence and the students’ perceived control of quitting tobacco use. The sixth session described the period of adolescence and the role of self-identity in embracing or rejecting certain behaviors, such as tobacco use. The seventh and eighth sessions explored self-diagnosis and discussed students’ strengths, interests, fears, goals, and expectations. The ninth session was a recap of the reasons why adolescents use tobacco, the perceived barriers of not using tobacco, and strategies that help prevent tobacco use. This session also taught students how to cope with negative behavior influences and exercise refusal skills. The tenth and final session summarized all of the previous lessons and had students draft and present a declaration to not use tobacco.
Additionally, an educational booklet on tobacco was distributed to the students during the first week of the program. A parent newsletter was sent home weekly for four weeks to inform the parents about the program and encourage family discussions about tobacco. Short anti-tobacco statements were broadcasted by the school during the students’ daily assemblies throughout the entire program delivery period. Finally, the students were encouraged to draw a picture at home that represents the adverse effects of tobacco use. The students’ artwork was displayed in the classroom on the last day of the program.
Program training and implementation
The curriculum instructors attended a 3-day training workshop about the content and delivery of the curriculum to familiarize them with the educational methods and tools employed during each session. They were coached by the program developer and by a certified trainer in communication skills, who was also the former regional director of education in Jeddah. A course book explaining the objectives and methods of teaching for each session was handed to each instructor. During the actual delivery of the program, the program developer met with the instructors on a weekly basis to review the educational material of the week and reinstruct them on teaching methods and tips.
Given the cultural makeup of Saudi Arabia and its gender-segregated schools, female dentists taught the curriculum to the female students and the program developer was able to observe and evaluate most of the sessions. The content and delivery of the curriculum were the same for all intervention classes. The instructors met with the participating students in the intervention schools twice a week for five continuous weeks to deliver the curriculum. Each session lasted about an hour. The sessions were instructed in an interactive way allowing frequent discussion with the students individually and among their respective groups. Information about anti-smoking clinics, which are funded by the Ministry of Health and provide free consultation and prevention services, were provided to students at the end of each session.
Questionnaire development
We applied the TPB, as detailed by Ajzen13,16, in developing our questionnaire to assess knowledge about tobacco and behavioral, normative, and control beliefs that affect tobacco use. The questionnaire development was guided by a previous research study of attitudes, beliefs, and subjective norms of tobacco use among adolescents in Saudi Arabia10. The questionnaire was originally developed in English and translated into Arabic, and the translation fidelity was established through a back-translation method. Finally, a group of middle school students, who were not part of the study population, were invited to the dental school to take part in a discussion of tobacco use and pre-test the questionnaire for content and clarity. The questionnaire was modified as suggested and prepared for pre- and post-testing among the study population.
Pre-test and post-intervention surveys
A baseline pre-test questionnaire was administered to the participating seventh-grade students in both intervention and control schools. The questionnaire was nearly half an hour long and was conducted under the supervision of the trained instructors. The students were reassured that the information collected in the survey was highly confidential, and the teachers were not permitted to enter the classrooms while surveys were being administered.
Following the complete delivery of the curriculum to intervention group participants, we administered two postintervention surveys, the first one was collected one week post-intervention (immediate) and the second was collected two years post-intervention, when the students were in their final year of middle school. Originally, we had also planned to administer the post-intervention surveys during the midpoint, when the students were in 8th grade. However, due to logistical reasons, only two post-test surveys were collected from study participants. The data were entered into an access database and later converted into SAS (version 9.4) for analysis.
Study measures
Sociodemographic characteristics and school-related measures
Data on student’s age, sex, school daily allowance, academic performance in previous year, absenteeism, religiosity, and parents’ level of education were collected. For analytical purposes, parents’ education was coded as <high school diploma, high school diploma, and >high school diploma. Academic performance in the previous year was coded as follows: 1, if student’s work consistently met grade level expectations; 2, if progress has been made but there is room for improvement; or 3, if there was a reason for concern. Absenteeism was assessed by asking students about their rate of skipping classes in a typical term: never, occasionally, sometimes, or most times. Absenteeism was coded as yes, if a student reported ‘sometimes’ or ‘most times’, and no if otherwise. Religiosity was scored on a 5-point scale, 5 being very religious and 1 not religious at all. It was recoded as religious if a student’s score was 5 or 4, and not religious otherwise.
Outcome measures
Self-reported current tobacco use, our primary outcome, was assessed using a dichotomous, yes/no question, ‘Do you currently use any form of tobacco?’. Secondary outcome measures were knowledge, attitudes, and perceived behavioral control (PBC).
The student’s knowledge about tobacco was assessed by asking 15 true/false questions. For example, ‘Smoking is harmful only if you smoke for a long time, 20–30 years or more’. A high score indicated better knowledge about tobacco.
Attitude was defined as the degree to which an individual has a favorable or unfavorable appraisal of a behavior. Direct attitude towards ‘not to use tobacco’ was measured with three items using a five-point bipolar scale: ‘For me, not to use tobacco is: unpleasant (1) / pleasant (5), bad (1) / good (5), and worthless (1) / valuable (5). Higher scores represented a positive attitude toward ‘not to use tobacco’. The Cronbach’s alpha measure of reliability was 0.70. The behavioral beliefs and corresponding outcome evaluation (indirect attitude) were developed from a previous study10. The behavioral beliefs were measured with five items based on a 5-point scale ranging from 1 (very unlikely) to 5 (very likely). The corresponding five outcome evaluation items were assessed on a 5-point scale ranging from 1 (extremely bad) to 5 (extremely good). Each behavioral belief item score was multiplied by its corresponding outcome evaluation to yield a weighted belief score. The higher the score, the more favorable the behavioral belief is toward ‘not to use tobacco’.
The PBC is the perception of how easy or difficult it is for one to perform the behavior. It was measured using 6 items rated on a 5-point scale, for example: ‘For me not to use tobacco is very difficult (1) / very easy (5), impossible (1) / possible (5)’; ‘I am confident that I will not use tobacco, strongly disagree (1) / strongly agree (5)’; ‘There is very little I can do to make sure that I do not use tobacco, true (1) / false (5)’; ‘It is entirely up to me not to use tobacco in the future, strongly disagree (1) / strongly agree (5)’; ‘How much control do you have over not to use tobacco? Absolutely no control (1) / complete control (5)’. The higher the PBC score the greater the sense of control over not using tobacco. The Cronbach’s alpha statistic was 0.66.
The study was registered in ClinicalTrials.gov as a retrospective trial and the identifier number is: NCT03579355 and adheres to CONSORT guidelines. The protocol of this study was approved by the Ethics Committee of the Deanship of Scientific Research at King Abdulaziz University, Jeddah, Saudi Arabia. Written study approval was also obtained from the Director of the Department of Education in Jeddah, and verbal consent was obtained from the participating students. The requirement for parental consent was waived by the ethics committee.
Student satisfaction survey
To identify the level of student satisfaction with the program, we developed several questions (total 25 questions) about the curriculum (lectures, videos, instructors), school tobacco broadcast, and other components of the program. The students were asked to rate whether each session of the program has helped them understand the topic using a 5-point scale with endpoints labeled ‘strongly disagree’ (1) / ‘strongly agree’ (5). The survey was administered to the students at the end of the program curriculum.
Statistical analysis
The Statistical Analysis Software (SAS, 9.4 version) was used to analyze the data. Descriptive statistics were generated for univariate and bivariate analysis that compared the intervention and control schools across a range of measures. Cohen’s effect size was calculated for knowledge and attitude outcome measures: sizes of 0.20 are small, 0.50 are medium, and 0.80 are large17. We utilized paired sample t-test for bivariate comparisons for continuous outcomes and chi-squared test for categorical outcome comparison between the two groups (intervention and control). For discreet or skewed distributions (e.g. knowledge and attitude), we employed the Wilcoxon rank-sum test, also known as the Mann–Whitney U test.
We used a mixed modeling approach for multivariate analyses. A mixed model is a statistical model containing both fixed and random effects. We ran two separate analyses to analyze our data, because we had both categorical (tobacco use) and non-categorical (knowledge, attitudes, and PBC) outcomes in our study. We used Proc Glimmix procedure for our categorical outcome (tobacco use) and calculated odds ratios and 95% confidence intervals. We used Proc Mixed procedure for non-categorical discrete variables (knowledge, direct attitude, indirect attitudes, and PBC) and reported the coefficient for component linear regression and its standard error. We modelled the study outcomes of individual students (level 1) while simultaneously assessing the influence of characteristic features of the schools that the participating students attended (at level 2). All tests of hypothesis were two-tailed and α=0.05. Finally, the means and standard deviations for each statement in the student satisfaction survey and overall scores were calculated.
RESULTS
Overall, the 10 sessions of the DFND curriculum were implemented as planned, with one modification, which was to combine sessions 7 and 8 into one. The students were delighted to meet the instructors, fully engaged in the class, and contributed positively to the discussion and content of the session. The mean students’ satisfaction score with curriculum sessions was 4.79/5 (SD=0.64), overall satisfaction with instructors was 4.78/5 (SD=0.67), and if they thought the program was helpful in preventing adolescent tobacco use was 4.78/5 (SD=0.75). The overall student satisfaction’s score with the program was 4.72/5 (SD=0.74) and about 80% reported listening to the school tobacco broadcast program with a mean satisfaction score of 4.2/5 (SD=1.17).
Study population characteristics
The baseline sample comprised of 371 participants (Table 1). The rate of absenteeism was higher among students in the intervention schools compared to their peers in the control schools (28.6% vs 18.5%; p<0.05). Students in the intervention schools had about three times the rate of tobacco use compared to those in the control schools (8.9% vs 3.0%; p<0.05).
Table 1
Baseline descriptive statistics of study participants in intervention and control groups (N=371)
| Variables | Intervention (N=203) Mean (SD) / n (%) | Control (N=168) Mean (SD) / n (%) | p |
|---|---|---|---|
| Age (years) | 13.22 (0.85) | 13.16 (0.84) | >0.05a |
| Parent education | |||
| <High school | 104 (51.23) | 75 (44.64) | >0.05b |
| High school | 42 (20.69) | 41 (24.40) | |
| >High school | 41 (20.20) | 37 (22.02) | |
| Don’t know | 16 (7.88) | 15 (8.93) | |
| School performance | |||
| 1 | 178 (87.68) | 145 (86.31) | >0.05b |
| 2 | 20 (9.85) | 14 (8.33) | |
| 3 | 5 (2.46) | 9 (5.36) | |
| Absenteeism | |||
| No | 145 (71.43) | 137 (81.55) | 0.02b |
| Yes | 58 (28.57) | 31 (18.45) | |
| Student allowance | 3.99 (1.52) | 4.05 (1.63) | >0.05a |
| Religiosity | |||
| Not-religious | 98 (48.28) | 90 (53.57) | >0.05b |
| Religious | 105 (51.72) | 78 (46.43) | |
| Knowledge | 9.08 (1.88) | 9.09 (1.56) | >0.05c |
| Direct attitude | 13.07 (2.76) | 13.39 (2.52) | >0.05 c |
| Indirect attitude | 113.50 (21.01) | 113.20 (21.08) | >0.05c |
| PBC | 24.31 (4.90) | 24.45 (4.62) | >0.05c |
| Tobacco use | |||
| No | 185 (91.13) | 163 (97.02) | 0.02b |
| Yes | 18 (8.87) | 5 (2.98) | |
Immediate effects of the tobacco prevention program on study outcomes
A total of 349 (94.1%) students completed the first post-test survey; 195 and 154 in the intervention and control schools, respectively. The bivariate analysis of the immediate effects of the DFND program at one week post-intervention is presented in Table 2. The mean score for knowledge about tobacco was 1.6 points higher among students in intervention schools compared to those in control schools (μ = 10.6, SE = 1.94 vs μ = 9.0, SE = 1.75; p<0.0001). Similarly, the mean score for students’ attitude beliefs about not to use tobacco was 7.1 points higher among students in the intervention schools compared to their peers in the control schools (μ = 122.6, SE = 30.25 vs μ = 115.5, SE = 27.89; p<0.05). Cohen’s effect sizes for knowledge and attitude were 0.89 and 0.24, respectively. Tobacco use decreased substantially by 36 percentage points from 8.9% to 5.6% in intervention schools but remained relatively the same in control schools (from 3.0% to 3.3%).
Table 2
Unadjusted immediate post-test results of school-based tobacco prevention program on outcome measures (N=349)
| Variables | Intervention (N=195) Mean (SD) / n (%) | Control (N=154) Mean (SD) / n (%) | p |
|---|---|---|---|
| Knowledge | 10.63 (1.94) | 8.99 (1.75) | <0.0001a |
| Direct attitude | 13.76 (2.23) | 13.40 (2.74) | >0.05a |
| Indirect attitude | 122.60 (30.25) | 115.50 (27.89) | 0.02a |
| PBC | 25.01 (5.05) | 24.79 (5.06) | >0.05a |
| Tobacco use | 11 (5.64) | 5 (3.25) | >0.05b |
Table 3 shows the results of the multilevel regression analysis of the immediate effects of the tobacco prevention program. The tobacco program improved knowledge about tobacco (β = 1.65, SE = 0.33; p<0.01) and indirect attitude towards not to use tobacco (β = 7.26, SE = 3.11; p<0.05) at one week post-intervention, after adjusting for other variables. There was no difference in tobacco use between intervention and control groups (OR = 2.10; 95% CI: 0.43–10.26).
Table 3
Multi-level analyses of immediate post-test effects of school-based tobacco prevention program on primary and secondary outcome measures (N=349)
| Variables | Knowledge Estimate (SE) | Direct attitudes Estimate (SE) | Indirect attitudes Estimate (SE) | PBC Estimate (SE) | Tobacco use OR (95% CI) |
|---|---|---|---|---|---|
| Group | |||||
| Intervention | 1.65 (0.33)b | 0.38 (0.26) | 7.26 (3.11)c | 0.38 (0.54) | 2.10 (0.43–10.26) |
| Control | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Parent education | |||||
| High school | 0.31 (0.25) | -0.12 (0.33) | 0.67 (3.98) | 0.61 (0.69) | NA |
| >High school | 0.30 (0.26) | 0.17 (0.33) | -0.61 (4.05) | 0.97 (0.70) | NA |
| Don’t know | -0.27 (0.35) | 0.54 (0.46) | -1.96 (5.61) | 0.55 (0.97) | NA |
| <High school | Ref. | Ref. | Ref. | Ref. | NA |
| Academic performance | |||||
| 1 | 0.39 (0.53) | 2.99 (0.70)a | 26.85 (8.46)b | 2.27 (1.46) | 0.18 (0.03–1.10) |
| 2 | -0.57 (0.61) | 1.99 (0.79)b | 27.87 (9.62)b | 1.52 (1.66) | 0.10 (0.01–1.40) |
| 3 | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Absenteeism | |||||
| Yes | -0.19 (0.23) | -0.92 (0.30)b | -9.82 (3.66)b | -2.09 (0.63)b | 2.44 (0.82–7.32) |
| No | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Allowance | -0.04 (0.06) | -0.05 (0.08) | 0.20 (0.99) | -0.11 (0.17) | 1.29 (0.95–1.76) |
| Religiosity | |||||
| Religious | -0.16 (0.20) | -0.16 (0.26) | -1.43 (3.15) | 0.15 (0.54) | 0.16 (0.03–0.74) |
| Not-religious | Ref. | Ref. | Ref. | Ref. | 1.00 |
Two-year post-test effects of the tobacco prevention program on study outcomes
A total of 278 (74.9%) students completed the second post-intervention survey 2 years post-intervention; 163 and 115 in intervention and control schools, respectively. Table 4 presents a significant difference in the unadjusted prevalence of tobacco use between intervention and control participants at two years post-intervention (19.6% vs 10.4%; p<0.05). From baseline, the unadjusted prevalence of tobacco use increased by 121 percentage points among participants in the intervention schools and by 250% percentage points among participants in the control schools. None of the other study outcomes was different at two years post-intervention. Cohen’s effect sizes for knowledge and attitude were 0.07 and 0.09, respectively. Table 5 displays the results of the multilevel regression analysis of the two years post-intervention effects of the tobacco prevention program. The difference in the likelihood for tobacco use between intervention and control schools was no longer significant after adjusting for covariates (OR = 0.77; 95% CI: 0.07–8.37).
The intention to use tobacco in the future between the intervention and control groups, immediately after the intervention, was not significant (p=0.96). Two years after the intervention, there was some changes in future intention to use tobacco, however, the change in intention did not reach statistical significance (p=0.09).
Table 4
Unadjusted two-year post-test results of school-based tobacco prevention program on outcome measures (N=278)
| Variables | Intervention (N=163) Mean (SD) / n (%) | Control (N=115) Mean (SD) / n (%) | p |
|---|---|---|---|
| Knowledge | 10.40 (1.52) | 10.29 (1.50) | >0.05a |
| Direct attitude | 13.85 (1.98) | 13.95 (2.02) | >0.05a |
| Indirect attitude | 98.09 (26.03) | 100.20 (23.27) | >0.05a |
| PBC | 24.15 (4.43) | 24.81 (3.57) | >0.05a |
| Tobacco use | 32 (19.63) | 12 (10.43) | 0.04b |
Table 5
Multi-level analyses of two-year post-test effects of school-based tobacco prevention program on outcome measures (N=278)
| Variables | Knowledge Estimate (SE) | Direct attitudes Estimate (SE) | Indirect attitudes Estimate (SE) | PBC Estimate (SE) | Tobacco use OR (95% CI) |
|---|---|---|---|---|---|
| Group | |||||
| Intervention | 0.18 (0.18) | 0.05 (0.25) | -2.11 (3.02) | -0.62 (0.52) | 0.77 (0.07–8.37) |
| Control | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Parent education | |||||
| High school | 0.17 (0.23) | 0.01 (0.31) | -0.80 (3.80) | 0.08 (0.64) | 1.26 (0.53–3.00) |
| >High school | 0.14 (0.23) | 0.21 (0.32) | -4.54 (3.84) | 0.27 (0.67) | 0.45 (0.15–1.33) |
| Don’t know | -0.30 (0.37) | -0.27 (0.52) | -1.41 (6.16) | -0.03 (1.07) | 2.33 (0.67–8.11) |
| <High school | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Academic performance | |||||
| 1 | 1.57 (0.53)a | 0.11 (0.75) | 6.87 (8.87) | -0.57 (1.55) | 0.72 (0.12–4.37) |
| 2 | 1.09 (0.58) | -1.44 (0.83) | -10.29 (9.83) | -4.03 (1.72)b | 0.68 (0.09–5.18) |
| 3 | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Absenteeism | |||||
| Yes | -0.37 (0.21) | -0.08 (0.29) | -1.28 (3.52) | -0.54 (0.61) | 1.77 (0.82–3.82) |
| No | Ref. | Ref. | Ref. | Ref. | 1.00 |
| Allowance | -0.06 (0.03)b | -0.02 (0.03) | -0.27 (0.43) | 0.01 (0.07) | 1.04 (0.96–1.13) |
| Religiosity | |||||
| Religious | -0.55 (0.18)b | 0.10 (0.25) | 2.18 (3.07) | 0.32 (0.53) | 0.99 (0.47–2.09) |
| Not-religious | Ref. | Ref. | Ref. | Ref. | 1.00 |
A comparative analysis between participants who were lost to follow-up in the intervention (20%) and control (30%) schools by tobacco use, was performed. The analysis of the 93 participants who completed the pre-test but were missing in the second post-test analysis showed no difference in baseline tobacco use between intervention and control schools (p>0.05).
DISCUSSION
In this study we implemented a comprehensive tobacco prevention program (DFND) guided by the TPB to prevent the initiation of tobacco use among seventh-grade female students in Jeddah, Saudi Arabia. Our findings suggest that our program was effective in increasing knowledge about tobacco, promoting attitudes towards not using tobacco, and in reducing tobacco use in the short-term. When we compared the prevalence of tobacco use at baseline (9%) with the prevalence at one week post-intervention (6%) in the intervention group, we observed a decrease in the prevalence of tobacco use by approximately one-third (36%). Among the participants in the control group, there was hardly any difference in the prevalence of tobacco use between baseline (3%) and at one week post-intervention (3%). The reduction in prevalence of tobacco use among participants in the intervention group (36%) is comparable to previous tobacco prevention programs of seventh-grade students that reported a short-term effectiveness in the range of 13% to 58%18,19.
Our short-term program effect size was large (0.89) for knowledge and small (0.24) for attitude. Our findings in this regard were also comparable to those reported by Hwang et al.20 in their review of 65 adolescent psychosocial smoking prevention programs, where the mean short-term effect sizes for knowledge and attitudes were estimated to be 0.53 and 0.22, respectively. The short-term gains in knowledge and attitude were lost after two years, which also agreed with Hwang et al.20 who reported a rapid decrease over time in program outcomes with large effect size magnitudes such as knowledge.
Our findings also showed a steady increase in the prevalence of tobacco use among female students over time. The proportion of current tobacco users in the intervention schools increased by 121% at two years post-intervention compared to baseline (from 9% to 20%). The increased prevalence of tobacco use was even larger among the controls; from 3% at baseline to 10% at two years post-intervention, an increase of 250%. This increase two years after the termination of the program is most likely explained by an increased uptake of tobacco use as the girls become older. Our findings are supported by the literature where significant increases in adolescents’ tobacco use occur with increasing age1, with the most remarkable increase around the age of 14 years21.
Despite the increase in tobacco use over time, the raw percentages of the effect of our tobacco program on the prevalence of tobacco use in the two groups at two years post-intervention showed some indication of residual program benefits (19.6% vs 10.4%; p<0.05). The prevalence of tobacco use increased threefold since baseline among the control group (from 3% to 10%), whereas it only doubled among the intervention group (9% to 20%). This finding is further supported by the results of the analysis of intention of future use of tobacco, which showed some evidence of a favorable change (p=0.09). The residual effect of our intervention on tobacco use, though not statistically significant after adjusting for covariates, concurs with findings of previous studies where small size effects on tobacco use persisted over time20. Reviews of school-based tobacco prevention programs found that the success of these programs in maintaining long-term reductions in tobacco use is generally related to being comprehensive, i.e. including community initiatives, and having larger magnitudes of immediate combined effects of knowledge, skills, and attitude11,12,22. In addition, sustained multi-level educational activities and behavioral skills across middle and high school years are vital for shifting social norms of tobacco use23.
Our findings have implications for public health policy. Effective and immediate comprehensive measures are needed to curb the epidemic of adolescents’ tobacco use24. Developmental school-community-incorporated programs that target adolescent females throughout middle and high school years are the most effective in reducing tobacco use20,22,25. Denormalization, transforming smoking into an increasingly socially unacceptable activity through media campaigns, health promotion programs, and smoking bans are effective in reducing tobacco use17,26. Furthermore, opening and promoting alternative social activities for Saudi girls, such as participation in social and cultural clubs, sports, and extracurricular activities may serve as an effective strategy in changing social norms of tobacco use27.
Strengths and limitations
Our study provided valuable longitudinal data to the existing knowledge about tobacco use among female adolescents. The study utilized the TPB to guide the development of study questionnaires and employed appropriate statistical analysis techniques. Our study had limitations. First, sample size calculation was not performed for this study, as it was designed as a pilot study. Second, baseline differences in tobacco use between the intervention (9%) and control (3%) schools indicate possible selection bias due to the sub-optimal selection of schools. Had the control and intervention schools been comparable at baseline in tobacco use, the impact of our program may have been more compelling. Third, more accurate projections on the effectiveness of the interventions would have been produced had we not missed the mid-program evaluation point (at 12 months post-intervention). A reporting bias may have partially contributed to the reduction of the prevalence of tobacco use in the intervention sample at the immediate post-test. However, we cannot verify with confidence the degree of this bias. Finally, the overall attrition rate was about 25% at two years post-intervention. The attrition analysis, however, showed no difference by tobacco use at baseline between participants who completed the study and those who did not. These limitations may have generally moderated the impact of our pilot program in observing a significant difference in tobacco use between the intervention and control groups over time.
CONCLUSIONS
Our study contributes to the existing knowledge about tobacco use and documents a steady increase in tobacco use among adolescent females in Saudi Arabia. Findings suggest that designing developmental school-based tobacco programs for adolescent females is feasible and when carefully implemented can be effective in increasing knowledge about the adverse health effects of tobacco use, promoting attitudes towards not using tobacco, and reducing intentions and initiation of tobacco use.